
In this section:
- Biological explanations of OCD: Genetic
- Lewis (1936) – families with OCD
- Nestadt et al (2010) twins and OCD
- Diathesis stress model
- Mutated genes: SERT gene & COMT gene, polygenic
- Neural explanations of OCD
- Understand how neurons transmit messages to each other
- The role of serotonin and dopamine in explaining OCD
- The worry circuit: orbit frontal cortex, thalamus, caudate nucleus
- Biological treatments for OCD: how SSRI’s and SNRI’s reduce symptoms of OCD
- Maria et al (2001) – symptoms of OCD return when medication stops
- Cromer et al (2007) behaviourist explanations
- Soomro et al (2009) effectiveness of drug treatments
Exam Tip: If you are asked about the genetic explanations, you should only refer to the COMT and SERT gene, and how OCD runs in families. You can mention that the gene effects low levels of serotonin and high levels of dopamine, but stop there! When talking about neural explanations, you should explain how dopamine and serotonin work at synaptic transmission, and the sum of neurotransmitters.
Biological Explanations of OCD
There should be no surprises here. The biological model, true to form, believes OCD to be the result of either genes, neurochemistry or brain structure. Keep in mind, if there is an issue with brain chemistry or brain structure then it’s our genes that would have caused this first and foremost.
Genetic explanation
No psychological disorder is entirely genetic bur some appear to be more genetic than others. OCD seems to fall into the category of high level of heritability.
There is clear evidence that OCD runs in families. Lewis (1936) Found that 37% of individuals with OCD had one or more parents with the disorder, and 21% had siblings with the disorder. Compare these figures to the 2% incidence of OCD in the general population and there is clear evidence of something genetic going on.
As always with family studies of this sort we cannot rule out environmental and social factors. Family members, brothers and sisters, parents and offspring, don’t just share genes but also living environment. It is quite likely that some of this concordance is down to nurture.
Nestadt et al 2010 looked at the concordance rate for Monozygotic (identical) and Dizygotic (Non-identical) twins with OCD.
MZ had a 68% concordance rate – this means if one twin had OCD, 68% of the time, the other twin also had OCD. DZ had a 31% concordance rate.

Mutated Genes – Genetic explanations
These are some mutated genes that predispose the development of the disorder.
For example the SERT gene is implicated in the efficiency of transporting serotonin across synapes. Serotonin plays a huge role in mood and social behaviour. If the SERT gene is mutated, it could result in lower levels of serotonin, and this variation has been linked to patients with OCD.
The COMT gene is involved in regulating the neurotransmitter dopamine. If the COMT gene is mutated, it could result in higher levels of dopamine and this variation is more common in patients with OCD, in comparison to people without OCD.
In the case of OCD, there seems to be hundreds of genes associated with the disorder. OCD is therefore said to be polygenic, as it is not possible to prove that OCD is caused by one faulty/mutated gene, but instead, a combination of mutated genes.
Evaluation of Genetic Explanations of OCD
Strengths:
- Research to Support = Validity: There is supporting evidence to suggest that OCD has a genetic influence. Nestadt et al (2010) looked at the concordance rate for Monozygotic (identical) and Dizygotic (Non-identical) twins with OCD. MZ had a 68% concordance rate – this means if one twin had OCD, 68% of the time, the other twin also had OCD. DZ had a 31% concordance rate. The research uses the IV of the type of twin, and found that individuals with identical genes have much higher rates of OCD. This enables the research to establish cause and effect and therefore improve validity.
- Deterministic explanations lead to Useful applications: Due to the biological explanations of OCD, this then lead to the development of drug treatments. Although it is not possible to target genes and change them, it is possible to target the effects that the genes have on neural activity. Soomro et al (2009) in a meta-analysis of 17 studies, found SSRI’s to be more effective in reducing symptoms of OCD, than placebo. However, they don’t work for everyone, 30% of patients reported no improvement and in the 70% who did, sometimes the improvements were slight. The fact that there is an improvement of symptoms with many individuals who suffer with OCD, help to provide support in the biological explanation. If neurotransmitters are balanced as a consequence of the drug, and the symptoms of OCD reduce, it seems plausible to suggest that there are biological contributors to OCD.
Weaknesses:
- Alternative explanations: Biological theories do not provide a full explanation. Mowrer’s two stage approach that we looked at in phobias can clearly explain some forms of OCD. A classically conditioned association between something like dirt or germs and anxiety or disgust. Negative reinforcement in the form of avoidance that prevents the patient ever facing up to the issue. It’s not surprising that some forms of systematic desensitization (behaviourist treatments) have been successful in treating patients with OCD. Diathesis stress model: One conclusion we can draw however; OCD is not entirely genetic, otherwise the concordance rate for MZ would be 100%. Other factors must therefore be involved. There appears to be a genetic predisposition, an increased likelihood of developing OCD that some people inherit from their parents. However, this doesn’t guarantee that OCD will develop. Other factors such as stress, upbringing, life events are needed to trigger the OCD. The Diathesis stress model offers an interactionist approach i.e. the influence of both nature and nurture.
- Nature/Nurture: It is impossible to separate nature from nurture, therefore they will both play a role in some shape or form. Cromer et al (2007) reported that about half of OCD patients could recall a specific, traumatic, event that may have triggered their OCD. Again this supports the idea that OCD is a result of a combination of nature and nurture.
- Lacks a holistic approach: OCD is complex and comes in many forms (hoarding, checking, tapping, illness, sexual, contamination). It’s unlikely that all of these will have the same cause. If it did, surely the same genes would cause the same symptoms. The fact that OCD is so varied, could suggest that other factors play a key role in OCD. However, this is not considered in the biological explanation. This reduces the validity of the explanation because it ignores the interaction between biology and social influence’s which undoubtedly have some role in OCD.
- Objective? Quasi-experiments: Research within this area tend to use twin studies to support genetic influence of OCD. However, this research has no control over nurture influences. Using quasi-experiments in this way, limits the control that the researchers have. Therefore, whether genetics and OCD have a cause and effect relationship can be questioned.
Neural Explanations:
For more of an intro do neurons and synaptic transmission go to Paper 2, biopsychology, neurons, neurotransmitters and synaptic transmission. Link to it below;
Neurons, Neurotransmitters & Synaptic Transmission
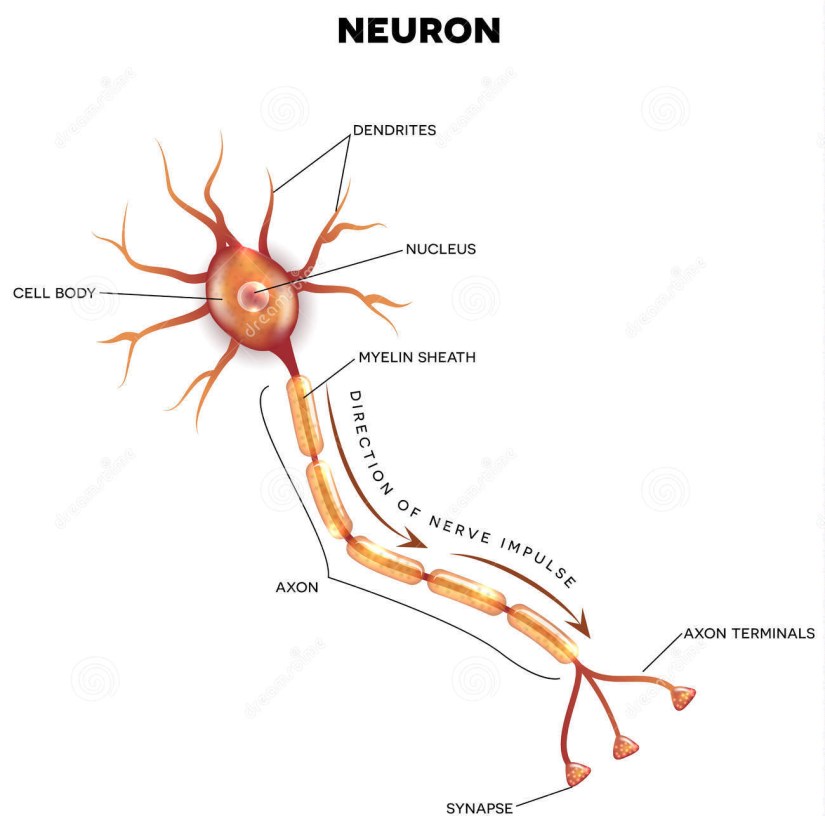
Neurons send messages to other neurons through an electrical impulse. Information from the senses (eyes, ears, skin, taste etc) are received and create an action potential in the neuron.
A neurotransmitter influences a neuron in one of two ways: excitatory or inhibitory.
An excitatory transmitter promotes the generation of an electrical signal called an action potential in the receiving neuron, while an inhibitory transmitter prevents it. Whether a neuron fires, depends on the sum of the neurons received. For example if there are more excitatory neurotransmitters in comparison to inhibitory, then the neuron will fire an electrical impulse down the axon of the neuron. If there are more inhibitory neurotransmitters in comparison to excitatory then the neuron is unlikely to fire an electrical impulse.
The main neurotransmitters you need to know are Dopamine and Serotonin. As you can see from the description below, serotonin is an inhibitor and dopamine is excitatory.
Inhibitory Neurotransmitters: If the neurons receptors receive more inhibitory neurotransmitters in comparison to excitatory, then the neuron is unlikely to fire an electrical impulse.
Serotonin is involved in the regulation of mood, it makes you calmer and more focused. Low levels of serotonin prevents the transmission of mood-related messages at the synapse. This is thought to be linked to anxiety and stress in OCD sufferers.
Excitatory Neurotransmitter: If there are more excitatory neurotransmitters in comparison to inhibitory, then the neuron will fire an electrical impulse down the axon of the neuron.
Dopamine an excitatory neurotransmitter and is a feel good chemical related to pleasure and reward systems. The increased dopamine is thought to be linked to compulsive behaviours in OCD sufferers.
What happens in the brain of someone with OCD?
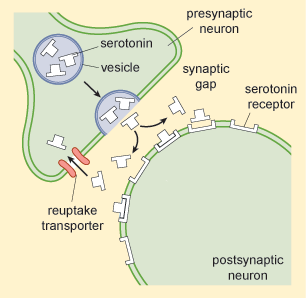
So in people with OCD, they have an increased amount of dopamine in their brains in comparison to a ‘normal’ brain. Therefore, when neurons send messages in the brain, their neurotransmitters are mainly excitatory (dopamine) which are sent via an electrical impulse which travels down the axon to the end of the presynaptic neuron. The electrical impulse forces the neurotransmitters (dopamine) out into the synapse. These neurotransmitters are then received by the receptors of the post synapse (this means the message has been received). Every time an individual with OCD carries out a compulsive behaviour, they are getting a surge of dopamine. This gives them a brief feeling of happiness (relief), but this happens again and again and again, and they become addicted. Their compulsions become a drug to them i.e. compulsion = dopamine hit.
On top of this, low serotonin has been linked to OCD, therefore, they do not have the right amount of the inhibitory neurotransmitter that helps them to help stabilize their mood and calm them down. If the sum of all the neurotransmitters are always in favour of dopamine, then they are constantly experiencing the effects of the dopamine, but are unable to feel the stabilizing effect of the serotonin.
Anyway, it is also important for you to understand what happens once the message has been received by the post synaptic neuron as this will help you to understand how drugs can work to reduce symptoms of OCD.
Once the message is received, the post synaptic neuron no longer needs the neurotransmitters. The post synapse then sends the neurotransmitters (dopamine) back to the pre-synaptic neuron, this is a process known as reuptake. This is so the presynaptic neuron can reuse the neurotransmitters (dopamine) again. Think of neurons as eco-friendly. They would never buy a single use plastic bottle! It’s just not the way they do things! They reason why neurons do this, is because if the neurotransmitters stayed in the synapse, they are likely to be destroyed by enzymes. So the pre-synaptic neuron, not only reuses them, they protect them too. If only humans were more like neurons ;-). However, this causes issues with people with OCD, as explained above. They are receiving dopamine in much larger volumes and this causes their compulsions to continue.
The worry circuit
The cycle of thoughts and actions in OCD might reflect a fault in an essential pathway in the brain. The pathway involved in obsessive-compulsive behaviour is a loop involving three anatomical brain regions. These are the:
- Orbital-frontal cortex
- Caudate nucleus
- Thalamus
The Orbitofrontal cortex (OFC) converts sensory information into thoughts and actions. This is the part of the brain that notices when something is wrong. For example, when the Orbitofrontal cortex registers that there is dirt nearby, it sends a ‘worry’ signal to the Thalamus.
If OFC could talk it would say “OMG! I’ve got something to worry about. The Thalamus needs to know about this”
In a normal functioning brain, the Thalamus receives the ‘worry’ signal, it becomes excited and sends strong signals to the Caudate Nucleus. The Caudate Nucleus acts like the brake pedal on a car, suppressing the original ‘worry’ signals. It tells the Thalamus that there’s no need to worry.
If the Thalamus could talk to the Caudate Nucleus it would say ‘Worry signal received’ and the Caudate Nucleus would say ‘Don’t worry, be happy’
But in OCD, the Caudate Nucleus is thought to be damaged, so it CANNOT suppress worry signals. This means that the Thalamus becomes over-excited.
In this case the Thalamus would say ‘Worry, worry, worry, worry!’ and the Caudate Nucleus would kind of ignore it and let it continue to worry.
The Thalamus then sends strong signals back to the Orbitofrontal Cortex which then turns this thought into an action. These actions relate to the compulsions experienced by those with OCD.
The Orbitofrontal Cortex would say “The Thalamus is really serious about this dirt. You need to wash your hands”
Evaluation of Neural Explanations of OCD
Strengths:
- Research to support: Fallon (1994) reported that 40% of people contracting Lyme’s disease (a bacterial infection spread by ticks) incur neural damage resulting in psychiatric conditions such as OCD. This suggests that the neural explanation can account for the onset of some cases of OCD. On the other hand, consider why it might be difficult to establish cause and effect between Lyme’s disease and OCD. On the other hand, it could be argued that the illness simply trigger symptoms in those who are more genetically vulnerable to OCD i.e. they already have the OCD candidate genes.
- Deterministic explanations lead to Useful applications: Due to the biological explanations of OCD, this then lead to the development of drug treatments. Soomro et al (2009) in a meta-analysis of 17 studies, found SSRI’s to be more effective in reducing symptoms of OCD, than placebo. However, they don’t work for everyone, 30% of patients reported no improvement and in the 70% who did, sometimes the improvements were slight. The fact that there is an improvement of symptoms with many individuals who suffer with OCD, help to provide support in the biological explanation. If neurotransmitters are balanced as a consequence of the drug, and the symptoms of OCD reduce, it seems plausible to suggest that there are biological contributors to OCD.
- Scientific/Objective data: Saxena (2000) reviewed studies of OCD that used PET scans, fMRI and MRI neuroimaging techniques to find consistent evidence of an association between the orbital frontal cortex brain area and OCD symptoms. This suggests that there are neural mechanisms involved in OCD.
Weaknesses:
- Nature/Nurture: It is impossible to separate nature from nurture, therefore they will both play a role in some shape or form. Cromer et al (2007) reported that about half of OCD patients could recall a specific, traumatic, event that may have triggered their OCD. Again this supports the idea of a diathesis-stress cause for the disorder.
- Lacks a Holistic Approach: OCD is complex and comes in many forms (hoarding, checking, tapping, illness, sexual, contamination). It’s unlikely that all of these will have the same cause. If it did, surely the same neural imbalance would cause the same symptoms. The fact that OCD is so varied, could suggest that other factors play a key role in OCD. However, this is not considered in the biological explanation. This reduces the explanatory power of the explanation because it ignores social influence’s which undoubtedly have some role in OCD. In addition, the cognitive approach can also be used to explain OCD. Gerig (2000) found that irrational thought processes of 9 OCD patients were associated with activity within the orbital frontal cortex in comparison to those without OCD. This illustrates how the neural and cognitive models can be combined to explain OCD.
Biological Treatments for OCD
All drugs, prescription and recreational have their effect at the synapse. They work by blocking the reuptake of neurotransmitters (e.g. serotonin, dopamine) so that the neurotransmitters can be received by the post synapse, again and again.
We saw in the last section that lowered levels of serotonin have been suggested as a possible cause of OCD. It should come as no surprise therefore, that drugs that help to encourage serotonin to remain in the synapse so that they are more effectively received by the post synapse.
SSRIs (Selective Serotonin Reuptake Inhibitors)
Serotonin is released from the pre-synaptic neuron and travels into the synapse. When it reaches the post-synaptic side it triggers receptors. If enough receptors are stimulated the message continues. Remember we talked about this earlier in neural explanations. This is known as an action potential. If the sum of neurotransmitters are more inhibitory neurotransmitters (serotonin) in comparison to excitatory then the neuron is unlikely to fire an electrical impulse.
A fraction of a second after release, the serotonin is sucked back into the presynaptic neuron ready to be recycled (reuptake). This reduces the levels of serotonin in the synapse. SSRI’s such as Proazac (fluoxetine), block the suction pumps and prevent the reuptake of serotonin. This means that the serotonin remains in the synapse, increasing the likelihood of the serotonin being received by the post synaptic neuron, again and again. This improves the likelihood that the sum of neurotransmitters, goes in favour of the inhibitor (serotonin). Because serotonin is now being received more, this means that the message of ‘regulating mood’ is more likely to be successfully received.
However, it is important to understand that SSRI’s do not increase the production of serotonin! They simply block the reuptake so that the serotonin builds up in the synapse.

SNRI’s (Serotonin and Noradrenaline Reuptake Inhibitors)
Evaluation of Biological Treatments of OCD
Strengths:
- Usefulness: Soomro et al (2009) in a meta-analysis of 17 studies, found SSRIs to be more effective than placebo. They do reduce the symptoms of OCD. However, they don’t work for everyone. 30% of patients reported no improvement and in the 70% who did, sometimes the improvements were slight.
- Holistic: Ideally drug treatments should be combined with therapy such as CBT. Drugs reduce some of the anxiety and mood-related symptoms allowing CBT to be more effective. Therapy on the other hand does attempt to tackle the underlying causes and is therefore seen as more of a cure, rather than a treatment.
- Useful Applications: Drugs are cheap. They may not appear to be so when you pay for your prescription each month, but they are certainly cheaper than therapy. Drugs require you to be diagnosed by a doctor and then you receive prescriptions. CBT requires a trained professional that you meet with for a large number of sessions which costly.
- Practical applications: Drugs are less time-consuming. It takes seconds to take a few pills, therapy may take an hour a week for many weeks. In addition, drugs are less disruptive to peoples lives. For example, people need to travel to hospitals or clinics for therapy. They may have to take time off work each week. When taking drugs, this is likely to be far less disruptive as it can be taken during an individuals daily schedule.
Weaknesses:
- Usefulness: Drugs reduce or remove the symptoms but don’t get to the root-cause of the problem. When we stop taking drugs the problems return. In the case of OCD, Maira et al (2001) found that symptoms return soon after medication is stopped. This can be a real problem in treating OCD. This could turn into a viscous cycle where the individual stops feeling their OCD symptoms and then stops taking the medication, but then the symptoms return and they start taking the medication again. Knowing that you need to take a drug to feel ‘normal’ can also be a tough pill to swallow and may be psychologically harmful.
- Individual differences & Usefulness: SSRI’s do not work immediately. It may be many weeks before there are noticeable improvements. Often in the first few weeks there may be issues with increased anxiety and insomnia. Not ideal when you already have anxiety from OCD. Many people stop taking them during this period which would impact the effectiveness of this treatment.
- Ethics – Psychological or Physical Harm: All drugs have side effects. They don’t just affect the pathways in the brain that you want them to target. Other pathways carrying out other functions are also affected. Typically SSRI’s bring dry mouth, constipation, blurred vision and erectile dysfunction (especially in men). The side effects of SNRI’s tend to be more common and more serious. Weight gain, erectile dysfunction, aggressiveness and issues with the rhythm of the heart are all side effects which can make people with OCD feel worse.
- Ethics – Deception: Psychopharmacology is the branch of medicine that deals with the effects of drugs on thinking, behaviour, mood etc. It is big business and worth billions of pounds a year. There is a strong vested interest to evidence that the drugs do work! As a result it is thought that research showing success tends to be favoured for publication. Studies that suggest the drugs don’t work tend to be either glossed over or ‘published in a way that conveys a positive outcome.’
- Alternative explanations: Drug treatments do not consider all contributing factors of OCD. Cromer et al (2007) reported that about half of OCD patients could recall a specific, traumatic, event that may have triggered their OCD. This could mean that drugs could be ineffective in treating individuals who have learned the symptoms of OCD. By only targeting serotonin levels, it may actually make the individual worse, as it has only been assumed that they have low levels of serotonin. But this may not be the case. Drugs should not be a one-fits all approach and individual differences must be considered in order to provide the most effective treatment.
