
Put your head phones in and experience what it is like to have auditory hallucinations
- Schizophrenia is a type of psychosis, a severe mental disorder in which thoughts and emotions are so impaired that contact is lost with external reality.
- Schizophrenia is the most common psychotic disorder, affecting about 1% of the population.
- Predominantly the illness affects younger people and 75% of sufferers will first experience the onset of schizophrenia between the ages of 16 and 25.
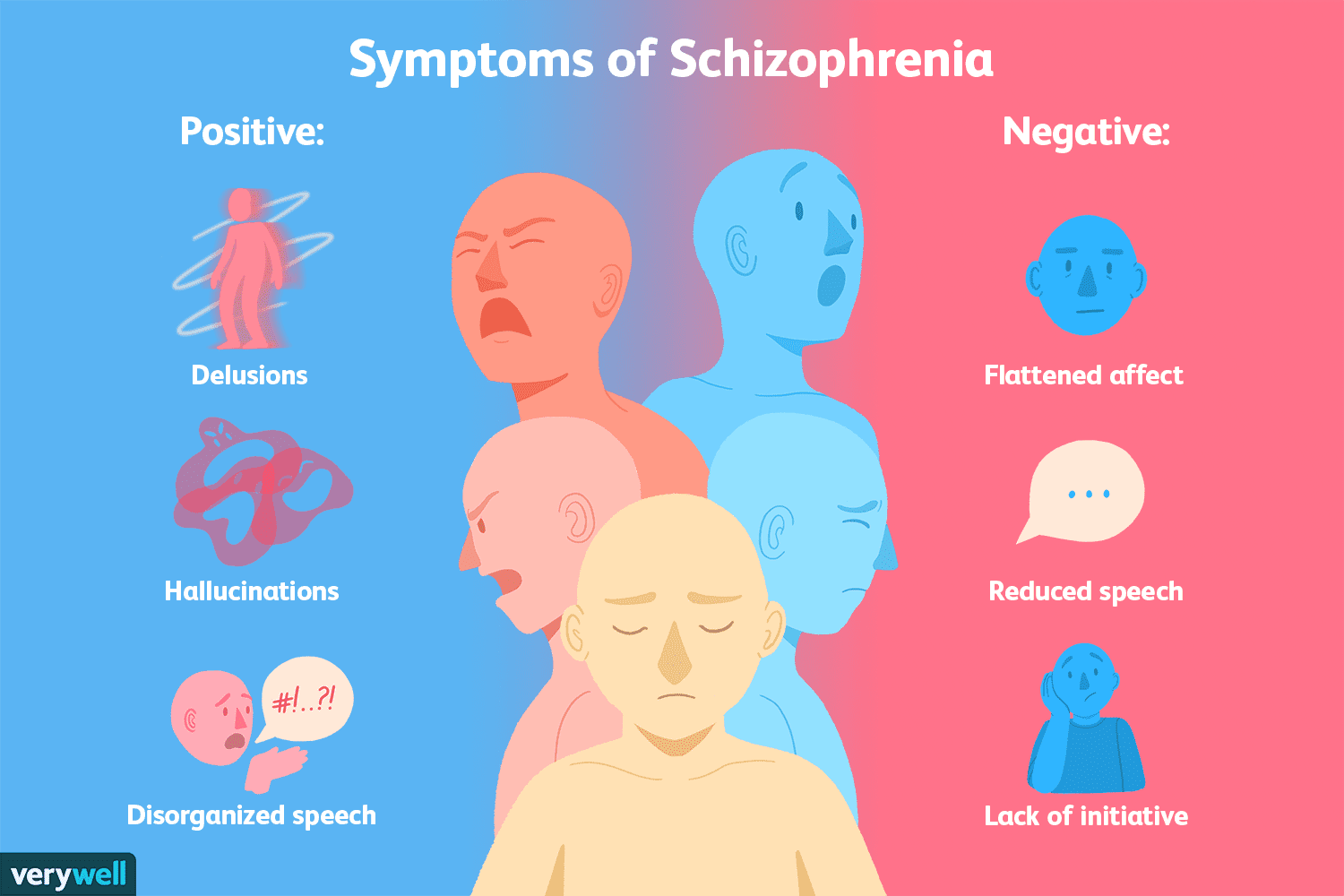
- Someone with schizophrenia can experience delusions (a belief in something that is not, nor could be, true) and hallucinations (experiencing stimuli/sensory information that are not present).
- There are many symptoms of the disorder, although not every patient displays all the symptoms.
This video was produced by a sixth form student and I think it takes a really empathetic approach in breaking down the stereotypes of the disorder, whilst also raising awareness.
Movies that showcase schizophrenia



Memory Strategy – SHADED
Speech Poverty
Hallucinations
Avolition
Delusions
Emotional Flattening
Disorganised Thinking
Positive Symptoms: Something extra e.g. a behaviour or biological reaction that you didn’t have before.
- Delusions – beliefs that conflict with reality. It can also be described as a fixed, false belief that an individual holds with absolute conviction, even when presented with clear, contradictory evidence.
- Disorganised Thinking – a severe disruption in the structure and formation of thoughts. It impairs a person’s ability to logically process, organize, and communicate information, making it difficult to maintain a coherent train of thought or follow a conversation.
- Hallucinations – mainly auditory or visual, but can be involve any of the senses.

Negative Symptoms: These reflect a reduction or loss of normal function.
- Speech poverty – a rambling of sentences that are difficult to understand, because there is a reduction in the quality of speech.
- Avolition/Apathy: inability to initiate in goal-directed behaviour e.g. poor hygiene, inability to work, lack of energy. Links to a depressive symptom.
- Emotional flattening – reduction in range and intensity of emotional expression, voice tone, eye contact and body language.
Evaluation: Issues when Diagnosing Schizophrenia
All of the following evaluation points are really important for you to know for the exam because each of the following are named on the specification:
- CO-MORBIDITY
- CULTURAL BIAS
- SYMPTOM OVERLAP
- GENDER BIAS.
This means that exam questions could have these words in them e.g. Discuss comorbidity and symptom overlap as issues in diagnosing schizophrenia (8 marks)
Essentially, this is one of the few topics where you should learn the evaluation points, because the specification is giving you specific ones to focus on.
- Point: One issue in the diagnosis of schizophrenia is comorbidity, which occurs when two or more disorders exist together. Evidence: Schizophrenia is frequently diagnosed alongside conditions such as depression and substance abuse. For example, Buckley et al. (2009) found that around half of schizophrenia patients also experience depression. Explain: This creates difficulties for clinicians because symptoms may be attributed to more than one disorder, making it unclear which diagnosis is most accurate. Consequence: As a result, the validity of schizophrenia as a distinct disorder is reduced, as it becomes difficult to distinguish it from other conditions, and patients may be misdiagnosed. Challenge?
- Point: Another issue is symptom overlap, where symptoms of schizophrenia are also present in other disorders. Evidence: For example, schizophrenic symptoms such as avolition and delusions can also occur in bipolar disorder. Explain: This overlap makes diagnosis difficult because clinicians may interpret the same symptoms differently. For instance, a god like mentality seen in bipolar, could be seen as a sign of a delusion in schizophrenia depending on the context. Consequence? Challenge?
- Point: A further issue is gender bias in the diagnosis, which highlight that schizophrenia may be diagnosed differently in males and females. Evidence: Research suggests that men are more likely to be diagnosed than women. For example, Longenecker et al. (2010) found higher rates of diagnosis in men, even when symptom presentation was similar. Explain: This may occur because diagnostic criteria are based largely on male symptoms, meaning female presentations—such as more emotional or affective symptoms—may be overlooked or misdiagnosed as mood disorders. Consequence? Challenge?
- Point: Finally, cultural bias is an important issue in diagnosing schizophrenia. Diagnosis often depends on cultural norms about what is considered abnormal behaviour. Evidence, Explain, Consequence, Challenge?
The video below is a very biased video about reliability issues. None the less, it gives you some insight into the inconsistency of diagnosis.
Extension – If you really want to show the examiners that you know your stuff, you could use these types of validity 😉
- Aetiological validity: the extent to which the cause of the disorder is the same for each sufferer.
- Descriptive validity: the extent to which individuals diagnosed with the same disorder are similar.
- Predictive validity: the extent to which the diagnostic categories predict the course and outcome of treatment accurately.
