
The specification states that you need to be able to explain, identify and evaluate each of the following methods of measuring the brain;
fMRI (small f, cap MRI)
EEG
ERP
Post mortem
All of which is explained below. Additionally I have included examples of research where this method has been used and what it can tell us. I would recommend you read these to help give you a bit more of a contextual framework to help your understanding.
You will also find that when you are learning more about the brain, you will come across evidence of these methods being used. You will be able to use your knowledge of the strengths and weaknesses of these different scans, to help you understand the research in some other areas of the specification.But I’ll refer back to this page when the time comes!
Introduction to brain imaging
There are many different approaches to understanding human thought and behaviour, but to really understand how the brain works, you need to look inside it. This is not as gruesome as it sounds, as many brain imaging methods today are entirely non-invasive.
However historically, clinicians relied on post mortem examinations. For example, a doctor called Broca was very interested in patients who lost their capacity for speech. He had a patient known as Tan, who had lost the ability to say anything other than the word ‘Tan’. Broca studied these patients, and then when they died he dissected their brains to search for areas that had noticeable damage. He located a region that appeared to be damaged in Tan and other similar patients. This was theorised to be the area responsible for language. To this day it is known as Broca’s area.
These days, we rely on scanning technology. Each type of scan has its own strengths and weaknesses.
Key terms
Temporal resolution = the accuracy of the scanner in relation to time, ie how quickly the scanner can detect changes in brain activity.
Spatial resolution = the smallest feature (or measurement) that a scanner can detect. Eg if a scan has a spatial resolution measured in cm, it can only detect brain activity to the nearest cm. If it has a spatial resolution measured in mm, it can detect which brain area is active much more accurately.
fMRI – functional magnetic resonance imaging
What is it and how does it work?
In an MRI machine, the patient has to lie still on a gurney which is in the middle of a strong magnetic field.
(Extra info for keen scientists: an MRI machine aligns most of the hydrogen atoms in your body in a particular way. Some aren’t aligned though, and these will absorb then release some energy. The energy they release, which is called the resonance, can be detected. Different tissues in your body have different resonances. This allows a complex picture to be built up of the different tissues in the body, a static ‘3D map’)
fMRI machines are specialist MRI machines that can show activity as it occurs. They work by monitoring the flow of oxygenated blood. This is possible because haemoglobin and oxyhaemoglobin have different magnetic properties (keen scientists: oxygenated blood and deoxygenated blood will resonate differently in the scanner). The magnetic resonance information is automatically processed by computer, and a series of scan pictures are generated by computer, showing the oxygenated blood flow in different areas of the brain
So – when a brain region is active, it will require more oxygen. The flow of oxygenated blood to that region will increase. Thus an fMRI scan can help us build up a picture of brain activity. The person having the scan can communicate with the technician verbally, and can be shown visual information, so they can carry out cognitive tasks while in the scanner. Blood flow in their brain is monitored while they carry out these tasks.
Key characteristics:
- Shows activity 1-4 second after it occurs (poor temporal resolution)
- Accurate within 1-2mm of the brain (good spatial resolution)
- Produces 3D images
- To buy the machine costs about £1.5 million, each scan costs about £400 to do.


Research in action
Your Brain Sees Even When You Don’t
A 2013 study published in The Journal of Neuroscience suggests that the brain can “see” someone else’s actions even when the ability to visually see has been destroyed. Cortical blindness refers to the loss of vision that occurs when the primary visual cortex no longer functions, generally as the result of injury. There’s no longer an ability to visually perceive the world in the sense with which we’re most familiar (even though the eyes still technically work), but that doesn’t necessarily mean the brain no longer sees.
In this study a patient with full cortical blindness could still react to another person’s gaze. While in an fMRI machine, the patient was exposed to gazes directed at him and gazes directed away from him. On the face of it, neither should matter — his visual cortex couldn’t perceive any sort of gaze. But the brain scan indicated that another part of his brain definitely could.
The patient’s amygdala, the brain area associated with figuring out whether external stimuli is a threat, showed a distinctly different activation pattern when the gaze was directed at the patient than when directed away from him. In other words, it didn’t matter that his visual cortex couldn’t catch the gaze—another part of his brain did regardless, and that’s quite incredible.
Article debating if FMRI can inform us on Cognitive Theories
Evaluation: CRRIED
Causation: A significant weakness of functional magnetic resonance imaging (fMRI) lies in the limited ability to draw causation conclusions from the data it provides. Unlike experimental methods that directly manipulate variables to establish causation, fMRI scans merely measure changes in blood flow associated with neural activity. For instance, increased blood flow in a particular brain region does not necessarily imply causation; it could be a result of various cognitive processes or external stimuli. This limitation restricts researchers from making definitive statements about the causal relationships between brain activity and behavior.
Resolution (temporal): Functional magnetic resonance imaging (fMRI) exhibits a weakness in its poor temporal resolution. fMRI has a temporal resolution on the order of seconds, meaning it cannot precisely track neural events that occur within milliseconds. The limited temporal resolution of fMRI poses challenges in studying changing cognitive processes, such as decision-making or language comprehension, where quick neural responses play a crucial role. In psychological research, this limitation underscores the importance of combining fMRI with techniques offering superior temporal resolution to achieve a more comprehensive understanding of cognitive processes and brain function.
Resolution (spatial) A strength of functional magnetic resonance imaging (fMRI) lies in its impressive spatial resolution. Studies have shown that fMRI can detect changes in brain activity at the level of millimeters. This can provide detailed insights into the anatomical localization of the brain. For example, fMRI can precisely pinpoint the activation of specific brain regions during cognitive tasks or emotional experiences. This spatial resolution allows researchers to map brain activity with high precision. In psychological research, the heightened spatial resolution of fMRI enables the identification of brain regions associated with various cognitive functions, emotions, and disorders.
Invasiveness: One notable strength of functional magnetic resonance imaging (fMRI) is its non-invasive nature compared to other neuroimaging techniques. This characteristic enhances the applicability of fMRI in psychological research, enabling investigations into neural processes underlying various cognitive functions and disorders while prioritizing participant well-being and ethical standards For example, PET scans would require a participant being injected with radiation and and EEG/ ERP would require a participant managing electrodes being attached to their scalp, which could be uncomfortable. An fMRi would only require laying in a small space for a period of time. Some patients can find it claustrophobic and noisy (the magnets in the machine clank loudly!) but overall the non-invasiveness of fMRI not only ensures participant safety and comfort but also facilitates larger sample sizes and longitudinal studies, as it is more feasible for individuals to undergo multiple scans.
Expense: One downside of using functional magnetic resonance imaging (fMRI) is its high cost. The actual device itself is expensive to purchase, maintain, and operate. This financial barrier limits access to fMRI technology for many researchers and institutions. The high expense of fMRI testing also restricts the sample size of studies, which can affect the generalizability and reliability of findings in psychological research. While fMRI offers valuable insights into brain activity and cognitive processes, its costliness hampers its widespread use and accessibility in psychological research.
Diagnosis: One notable strength of functional magnetic resonance imaging (fMRI) lies in its potential as a diagnostic tool. For instance, fMRI has been employed in various clinical settings to detect abnormalities in brain function associated with neurological and psychological disorders such as schizophrenia, depression, and Alzheimer’s disease. Through fMRI, researchers and clinicians can identify specific patterns of brain activity that are indicative of certain conditions, aiding in early diagnosis and treatment planning. This diagnostic capability enhances the utility of fMRI not only in clinical practice but also in psychological research. By explaining the neural picture of different disorders, fMRI contributes to a deeper understanding of their underlying mechanisms, paving the way for more targeted interventions and therapies.
Guardian Article on Lie Detection in FMRI’s
EEG – Electroencephalogram
What is it and how does it work?
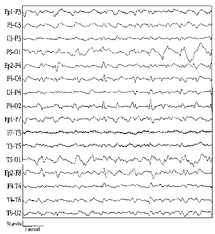
EEGs do not involve you being put into a machine, but require electrodes to be attached to the scalp. This can be seen in the picture below. Some machines are built to fit on like a swimming cap (called skull cap) and pick up the information they need from that.
They work by picking up on and recording the electrical activity of the brain. So, think back to when we learnt about neurons – remember, their function is to conduct electrical impulses. Each electrode works by detecting electrical activity immediately below it, so the more electrodes you have the more electrical activity can be picked up on. During a scan or reading you could have anything from 2-3 electrodes up to over 100 on your scalp. This provides an overall account of activity in the brain, as it tells you how much activity is going on and will identify the type of electrical activity that is happening.

Key characteristics
- Shows activity within milliseconds of the activity happening (good temporal resolution)
- The more electrodes there are the more accurate the reading: however, electrodes can only measure the activity at the surface of the brain, and cannot assess how deep the activity is, or where exactly it is happening. Also, a single electrode will be monitoring thousands of neurones in the brain area below the electrode, so activity can’t be narrowed down to specific neural connections (poor spatial resolution)
- And, as you can see above, the results of an EEG require a trained specialise to understand and interpret them.
Research in action
REM sleep and dreaming- Using EEGs
Evaluation – CRRIED
Point: A weakness of EEGs is that they do not provide information about causation, ie we cannot infer what is causing the brain activity seen.
Evidence: An EEG uses electrodes attached to the scalp that detect brain activity close to it. The brain will be process multiple things at once, and indeed sometimes we don’t even realize the brain is processing/ actioning a stimulus or behaviour.
Explain: While EEG detects changes in brain waves, it cannot determine whether these changes are caused by the stimuli being presented or other factors that are causing brain activity. It is impossible to determine what specifically is causing any reading or changes in readings.
Point: A weakness of EEGs is their poor spatial resolution.
Evidence: EEG electrodes measure electrical activity at the scalp surface.
Explain: Thus we can only learn the rough location of brain activity, as the EEG cannot tell us how deep within the brain it is occurring. Behaviours such as memory would be difficult to localise using this method due to the areas typically associated with memory being so far from the surface of the cerebrum.
Point: A strength of EEGs is their excellent temporal resolution.
Evidence: Due to the fact that the electrodes detect activity very quickly, an EEG offers excellent temporal resolution, capturing rapid changes in brain activity within milliseconds.
Explain: EEGs ability to track real-time brain changes allows researchers to see slight changes in activity as they happen. For example, slight changes in sleep stages or the pattern of an epileptic seizure, thus leading to a better understanding of that behaviour. In this respect they are better than fMRIs, which might miss rapid, transient changes.
Point: A strength of EEGs is their low cost in comparison to other methods of measuring the brain.
Evidence: In comparison to an FMRI, EEG equipment is relatively affordable and requires minimal maintenance. Unlike expensive neuroimaging techniques like fMRI or PET scans, EEG offers a cost-effective option for studying brain function.
Explain: The affordability of EEG technology expands opportunities for researchers to conduct large-scale studies, facilitating greater access to brain research across diverse populations and settings in psychology.
Point: A strength of EEGs is their usefulness in diagnosing certain conditions.
Evidence: EEGs are used clinically to diagnose various neurological conditions, such as epilepsy and sleep disorders, which show characteristic patterns of brain activity.
Explain: In psychology, EEG diagnostics aid in understanding the neural underpinnings of mental health conditions, informing treatment strategies and enhancing patient care.
ERP – event related potentials
What is it and how does it work?
These scans use the same equipment of EEGs, ie the electrodes and the ‘ponytail’ of wires leading to a computer, but they process the information in a more sophisticated way. This means that ERPs can tell us more accurately what is happening in the brain. On it’s own an EEG doesn’t actually tell us that much – the brain is processing so much information at any one moment that we can’t use an EEG reading to say a specific activity in the brain relates to a specific task or stimulus. To overcome this, the technology has been developed and the updated version is called an ERP scanner.
• Patients are presented with the same stimulus repeatedly (eg an image or a spoken word)
• The timing and type of stimulus is carefully controlled
• EEG readings are generated each time
• The electrical patterns are analysed statistically to identify the electrical activity associated specifically with the stimulus
• This means that ongoing background activity and noise can be accounted for
• The excellent temporal resolution of the EEG is maintained. Waves of electrical activity seen 100ms after stimulus show cognitive processing.
• Spatial resolution is improved to cm (but not mm, this is because the sensors are measuring activity at the surface, so signals are averaged across relatively large brain areas).
Research in action
Costa, Braun & Birbaumer (2003) used this method to record responses to nude pictures of both sexes in young people (19-29 years). When asked abut how they felt, men generally said they were aroused by the nude female pictures, whereas women mostly reported to having neutral feelings to both male and female pictures (self report measure- what could be a problem with this measure?). However, when the researchers examined the ERP’s, they found that participants had a much higher response to nude pictures of the opposite sex than they reported. Suggesting that this method of measuring activity is more accurate and less biased than other research methods adopted by psychologists.
A link to the original article can be found below:
Costa, Braun & Birbaumer 2003 ERP
Evaluation- CRRIED
As ERPs and EEGs use the same equipment the spatial and temporal resolution as well as how invasive it is would be evaluated in the same way as the EEG. The only difference is the questioning of causation. ERPs enable the determination of how processing is affected by a specific experimental manipulation. This makes ERPs use a more experimentally robust method as it can eliminate extraneous neutral activity, something that other scanning techniques (and EEGs) may struggle to do.
Causation. ERPs can detect brain responses to specific stimuli with high temporal precision. By analyzing ERP waveforms, researchers can infer the causal relationship between stimuli presentation and neural activity. This capability allows psychologists to investigate the mechanisms underlying cognitive processes and behaviors, advancing our understanding of brain-behavior relationships and informing interventions for cognitive disorders.
Temporal resolution. ERPs offer excellent temporal resolution, capturing rapid changes in brain activity within milliseconds. ERP’s ability to track real-time brain dynamics enables precise analysis of cognitive processes, including perception, attention, and decision-making. In psychology, ERP’s temporal resolution facilitates the investigation of dynamic brain activities underlying complex behaviors, contributing to a deeper understanding of human cognition and behavior in real-time contexts.
Spatial resolution. ERPs have limited spatial resolution compared to neuroimaging techniques like fMRI. ERP recordings measure electrical activity at the scalp surface, resulting in low spatial precision and difficulty in pinpointing the exact brain regions involved. The limited spatial resolution of ERPs restricts the ability of psychologists to precisely localize neural activity, which may limit insights into the neural networks underlying cognitive functions and behaviors.
Inconvenience. While not invasive, many people find ERPs inconvenient and restrictive. It require electrodes to be attached to the scalp, which can be uncomfortable for participants. It involves sitting still and repetition of tasks. This may limit long-term monitoring and may deter some individuals from participating in studies. In psychology, techniques like ERPs may restrict research participation and hinder the exploration of brain activity over extended periods, impacting the depth of understanding of cognitive processes and disorders.
Expensive. ERPs require minimal equipment and can be conducted using standard EEG setups. Compared to expensive neuroimaging techniques like fMRI or PET scans, ERPs offer a cost-effective option for studying brain function. The affordability of ERPs expands opportunities for researchers to conduct large-scale studies, facilitating greater access to brain research across diverse populations and settings in psychology.
Diagnosis. ERPs are used clinically to diagnose neurological disorders such as epilepsy and auditory processing disorders. By analyzing patterns of electrical activity, ERPs help clinicians identify abnormal brain function indicative of specific conditions. In psychology, ERPs aid in understanding the neural underpinnings of various disorders, informing diagnostic criteria and treatment strategies to improve patient outcomes.
Post mortem examinations
What is it and how does it work?
This method is probably the most familiar to you and also what you would imagine when thinking about a brain surgeon, something along the lines of the picture below!
This isn’t quite what a post mortem is – first of all, the patient needs to be dead for this to take place! Hence the name: ‘post’ means after, and ‘mortem’ means death. Clinicians will will open up the skull and examine the brain by observing and cutting into it with the aim of identifying any abnormalities that might explain the behaviours of people when they were alive. For example, they might examine the brain of serial killers or people with mental health issues to identify if there was anything in their brain structure that could be related to, or even cause the issues from their living life.
Key characteristics
- Not instant as all, as can only access the brain when the person is dead – therefore there is going to be an extreme time delay between the action and the post mortem.
- You can view the inactive brain in extreme detail, you would only be limited by the magnifying glass/ microscope you have access to.
Research in action
This is a example of where a post mortem revealed how different parts of the brain are responsible for different behaviours.
Link to a video: The Curious Case of Phineas Gage
Link to a case study example, Charles Whitman Mass- Shooter
Evaluation – CRRIED
Causation and temporal resolution: One of the main limitations of post-mortem examination is the issue of establishing causation. The deficit a patient displays during their lifetime (e.g. an inability to speak) may not be linked to the deficits found in the brain after death (e.g. a damaged Broca’s area). The deficits reported could have been the result of another illness, and therefore psychologists are unable to conclude that the deficit is caused by the damage found in the brain.
Another issue is that there are many extraneous factors that can affect the results/conclusions of post-mortem examinations. For example, people die at different stages of their life and for a variety of different reasons. Furthermore, any medication a person may have been taking, their age, and the length of time between death and post-mortem examination, are all confounding factors that make the conclusions of such research questionable.
Detailed examination (spatial resolution): However, one strength of post-mortem examinations is that they provide a detailed examination of the anatomical structure and neurochemical aspects of the brain that is not possible with other scanning techniques (e.g. EEG, ERP and fMRI). Post-mortem examinations can access areas found deep within the brain like the hypothalamus and hippocampus, which other scanning techniques cannot, and therefore provide researchers with an insight into these deeper brain regions. For example, Iverson found a higher concentration of dopamine in the limbic system of patients with schizophrenia which has prompted a whole area of research looking into the neural correlates of this disorder.
Invasive? While post-mortem examinations are ‘invasive’, this is not an issue because the patient is dead. However, there are ethical issues in relation to informed consent and whether or not a patient provided consent before his/her death. Furthermore, many post-mortem examinations are carried out on patients with severe psychological deficits (e.g. patient HM who suffered from severe amnesia) who would be unable to provide fully informed consent, and yet a post-mortem examination has been conducted on his brain. This raises severe ethical questions surrounding the nature of such investigations.
Alternative methods
Another comparison that can be made to the 4 methods above is a PET scan. This isn’t names on the specification so you CANNOT be asked specifically about this, however it might be worth knowing a little bit about it so you can use to explain any evaluative points you might make about the other methods above. Below is a link to a video explaining PET scans.
